
The Importance of Therapeutic Movement for our Older Clients
Nov 03, 2022
Periods of rest / immobilisation due to illness &/or injury, have the potential to amplify the deleterious effects of ageing on musculoskeletal tissue structure & overall functional capacity in older clients.
For many podiatrists, we are in a unique position due to our regular contact with older clients, where we may be able to effect significant change to help our older clients move more & age well.
When we think of exercise rehabilitation, quite often our minds will gravitate towards an active individual or athlete, who may wish to return to their sporting activities after an injury. Not often is a relatively inactive older individual the first client avatar that comes to mind in this scenario.
However, it is this client avatar where physical rehabilitation & functional restoration are arguably more important, when we are looking at the impact that periods of rest &/or immobilisation can have on long-term functional capacity and overall quality of life.
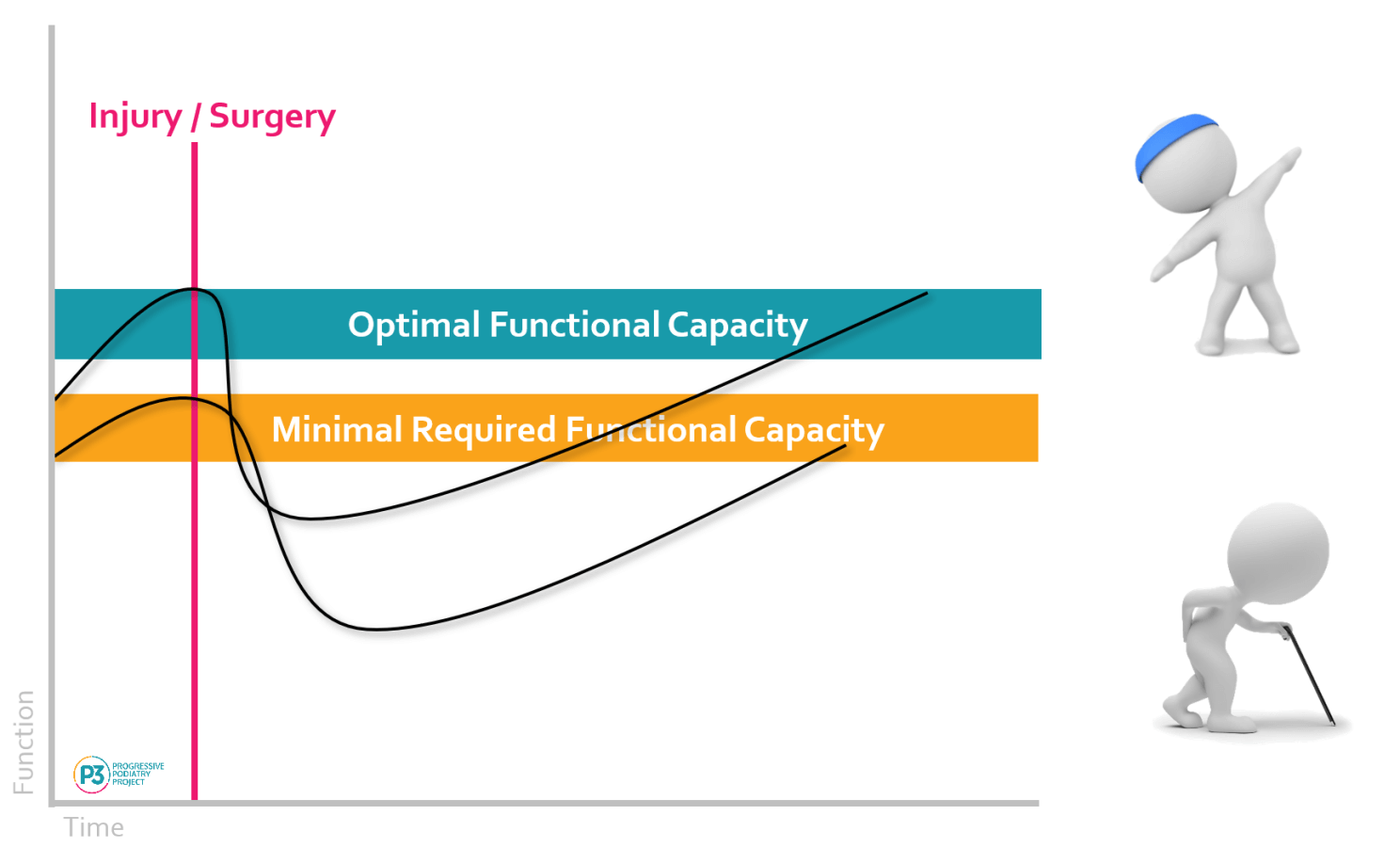
The Capacity Gap
One reason our minds follow this thought process is due to the capacity gap.
If we have a very active sporting person that has sustained an injury who wishes to return to high-performance activities, the capacity gap is quite obvious. It is easy to acknowledge that this individual will require some degree of physical therapy to restore their functional capacity to ensure safe return to their sport.
In contrast, if we have a relatively sedentary older individual that has sustained an injury, who simply needs to return to engaging in their activities of daily living, we can neglect to acknowledge the importance of physical therapy & functional restoration, due to the less-than-obvious capacity gap that presents.

For an older client, especially a relatively sedentary older client. even short periods of rest &/or immobilisation can have profound impacts on their functional capacity & quality of life, largely in part due to the amplification of senescence.
Senescence
Senescence = the natural deterioration of a cell / organism through the passage of time.
Healthy adult ageing of the human neuromuscular system is comprised of changes that include, but are not limited to, atrophy, weakness and slowed movements. Ageing alone does not account for the decreases in size and strength, with nutritional intake and reduced levels of physical activity further contributing to these reductions in tissue quality and function.
When we refer to the 'quality' of skeletal muscle, this refers to its composition, cellular structure & organisation, in addition to its ability to contribute to hormone regulation and the function of our immunometabolism.
From a cellular organisational & tissue composition standpoint, ageing skeletal muscle & tendons experience a reduction in elasticity, amplified by altered collagen cross-linkages - that impact the stiffness/compliance of the tissue. Skeletal muscle also experiences lipid & collagen deposition into the tissue. All of these changes influence the overall quality of skeletal muscle tissue and its aforementioned functions.
Two common terms used when referring to senescence & skeletal muscle are sarcopenia and dynapenia.
Sarcopenia refers to the reduction of muscle mass as we age. After 70 years of age we lose up to 1% of our skeletal muscle mass each year (Walston, 2014).
Dynapenia refers to loss of muscle strength, related to ageing and not caused by neurological or muscular disease. It is reported that we lose 10%-15% of muscle strength per decade, up to 70 years of age. After 70 years of age, this is accelerated to 25%-40% loss per decade (Clark & Manini, 2012).
Further expanding on function from a neurological standpoint, reduced spinal motor neurone output - as expressed by lower motor unit discharge rates (MUDRs) and deterioration of the sarcoplasmic reticulum, result in decreases in the speed of contraction and reduced force-generating capacity of skeletal muscle.
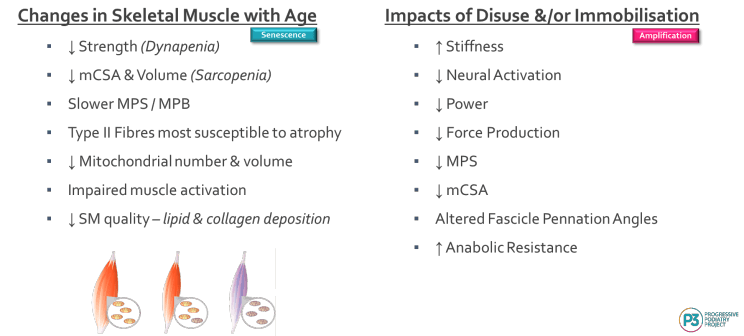
All of these aforementioned changes are natural and are what we could consider 'the bonus of having birthdays'. However, disuse, rest &/or immobilisation can considerably amplify these changes, significantly impacting our healthspan & quality of life (QOL).
Lifespan vs Healthspan
Lifespan refers to the total number of years we are alive.
Healthspan refers to how many of those years we remain healthy & free from disease.
Mechanical Unloading
Bed rest, immobilisation, lower limb unloading (eg: post-op shoe or moonboot) and even simply a decreased daily step count will contribute to amplifying the deleterious effects of ageing on skeletal muscle structure & function.
What's also easy to forget, is just how quickly periods of mechanical unloading can impact our muscle cross sectional area (mCSA), volume and force-generating capacity.
Even 5 days of immobilisation can see a 4% decrease in knee extensor mCSA & a 9% decrease in strength. Looking at longer periods of mechanical unloading, 84 days of best rest demonstrated a 17% reduction in vastus lateralis muscle volume and a 40% decrease in function (Gao et al, 2018).
Impact of Mechanical Unloading Relative to Age
Observed decreases in muscle size (volume/mCSA) are more profound in younger vs older individuals. Likely due to greater muscle protein synthesis (MPS) activity in younger individuals, as MPS attenuates with age.
However, the force-generating capacity of muscle more pronounced in older vs younger individuals. This is thought to be a result of decreased excitation coupling, partial denervation of muscle fibres and deterioration of the sarcoplasmic reticulum. As a result, the adaptive plasticity in skeletal muscle differs between young & old individuals.
What Can This Look Like Clinically?
For a younger individual who has been placed in a moonboot for 6-8 weeks, there may be a notable difference in calf muscle circumference compared to the contralateral limb. This will be due to their higher rates of muscle protein synthesis being attenuated due to the period of immobilisation (+/- nutritional &/or lifetstyle factors). The younger individual may also experience decreased force-generating capacity, but due to their age this may return after a short period of re-training.
For an older individual, who naturally experiences a decreased rate of muscle protein synthesis/muscle protein breakdown, less calf muscle atrophy may be observed. However, their force-generating capacity may be significantly impacted, potentially being unable to return to their pre-immobilisation level of function.
Given these differences, combined with a smaller capacity gap, it can be easy for clinicians to assume an older person doesn't require a post-immobilisation/post-mechanical unloading exercise program to improve/restore their functional capacity.
Further expanding on why our older client in this scenario may require more attention to improving their post-immobilisation functional capacity than we may have previously thought, is that as neuromuscular changes of the ankle plantarflexors play a very important role in the risk of falls in older people. Muscle weakness, gait & balance deficits are considered intrinsic risk factors, with the highest relative risk for falls in older individuals. As a result, ankle plantarflexor strength is considered an important predictor of functional decline in the older population (André et al, 2016).
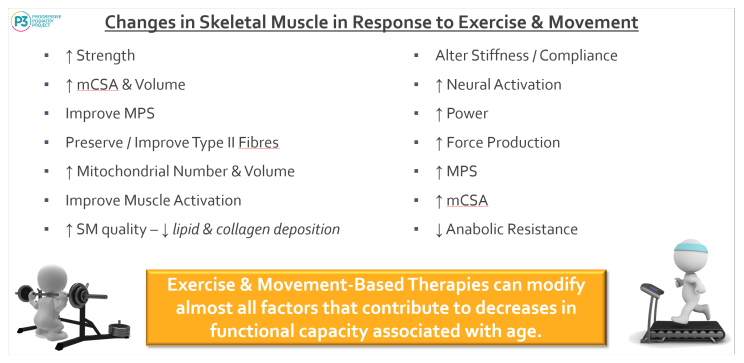
It's not all bad news, there are a number of observable changes we can see in skeletal muscle in response to exercise & movement, that can improve/restore functional capacity, even in our older clients.
Proactive vs Reactive
Our healthcare system is still arguably reactive as opposed to proactive. That is, we often take action after an adverse event has occurred.
If we take on a more proactive role, we can not only improve the healthspan of our clients, but also limit the extent and duration injury, illness &/or surgery can have on an individual's ability to function in their every-day life.
In our clinical practice there are a number of strategies we can adopt in order to help our older clients live & age well. These may include;
- Health Check / Monitoring - we perform annual neurovascular assessments for a number of clients, why not assess functional capacity too?
- Pre- & Post-Operative Assessments - if we are referring our patients for even 'minor' surgeries (eg: bunion correction or lesser toe procedures), a pre-op assessment can be highly beneficial in pre-op planning & post-op management.
- Post-Injury/Immobilisation Assessments - if we are aware that our clients have been ill or injured and have undergone a period of decreased activity, performing functional tests to assess their capacity relative to their age (or existing measures we have, if we have adopted annual functional tests).
No, I don't believe performing functional tests are outside of our scope and no, I don't believe we aren't equipped to prescribe our podiatric patients simple movement programs to help our older clients improve their functional capacity.
REFERENCES
Brook, M., Wilkinson, D., Phillips, B., Perez-Schindler, J., Philp, A., Smith, K., & Atherton, P. (2015). Skeletal muscle homeostasis and plasticity in youth and ageing: impact of nutrition and exercise. Acta Physiologica, 216(1), 15-41. doi: 10.1111/apha.12532
Clark BC, Manini TM. What is dynapenia? Nutrition. 2012 May;28(5):495-503. doi: 10.1016/j.nut.2011.12.002. PMID: 22469110; PMCID: PMC3571692.
D'Antona, G. (2003). The effect of ageing and immobilization on structure and function of human skeletal muscle fibres. The Journal Of Physiology, 552(2), 499-511. doi: 10.1113/jphysiol.2003.046276
Gao, Y., Arfat, Y., Wang, H., & Goswami, N. (2018). Muscle Atrophy Induced by Mechanical Unloading: Mechanisms and Potential Countermeasures. Frontiers In Physiology, 9. doi: 10.3389/fphys.2018.00235
Helô-Isa André, Filomena Carnide, Edgar Borja, Fátima Ramalho, Rita Santos-Rocha & António P Veloso (2016) Calf-raise senior: a new test for assessment of plantar flexor muscle strength in older adults: protocol, validity, and reliability, Clinical Interventions in Aging, 11:, 1661-1674, DOI: 10.2147/CIA.S115304
Siparsky, P., Kirkendall, D., & Garrett, W. (2013). Muscle Changes in Aging. Sports Health: A Multidisciplinary Approach, 6(1), 36-40. doi: 10.1177/1941738113502296
Suetta, C., Hvid, L., Justesen, L., Christensen, U., Neergaard, K., & Simonsen, L. et al. (2009). Effects of aging on human skeletal muscle after immobilization and retraining. Journal Of Applied Physiology, 107(4), 1172-1180. doi: 10.1152/japplphysiol.00290.2009
Walston JD. Sarcopenia in older adults. Curr Opin Rheumatol. 2012 Nov;24(6):623-7. doi: 10.1097/BOR.0b013e328358d59b. PMID: 22955023; PMCID: PMC4066461.
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
