
Do You Have Biomechanical Tunnel Vision?
Oct 12, 2022
Do you jump to a biomechanical assessment at a client's first mention of musculoskeletal pain?
Can this be short-changing your clinical outcomes? Let's discuss...
Now, let me be clear, I feel that a podiatrists' biomechanical knowledge, skills and ability to prescribe orthomechanical interventions are one of the many aspects of our profession that we can (and should) be proud of. However, I do feel that health practitioners (not just podiatrists) are often too quick to blame an individual's biomechanics (or other single-factors, eg: footwear) as the 'root cause' of a pathology/problem/clinical presentation, without having explored some of the arguably more important elements first.
I'm also not here to be critical or 'call out' anyone, my role as a coach & mentor is to help guide people through self-reflective practice, so that's what we're here to do, reflect.
Self-Reflection in Managing (Chronic) Plantar Heel Pain
If you are struggling to get consistently positive outcomes with your patients, I would suggest taking a step-back & consider how you are approaching your clinical history taking & management plan formulation.
Something is missing...

An Example...
I will often have coaching sessions with other health practitioners, to help put another set of eyes on a case. I can think of a few cases, all of which are quite similar - highlighting a bit of a trend, thus why we are having this discussion...
In these cases, I was approached by health professionals (I'm not just referring to podiatrists here) who typically had a patient with a really 'tricky and severe case of heel pain'.
The case histories I was provided with consisted of very little information that explored risk & predisposing factors, that would likely lead to devising an appropriate management plan. Instead I was provided with a list of arbitrary biomechanical measures and gait observations, that arguably could be a symptom of someone walking with heel pain or not relevant at all.
No information was provided regarding; activity history, occupational history, social history, pain pattern/history, diagnostic testing, functional testing, treatment/advice regarding management etc...
Does this sound familiar to you?
When we look at the identified risk factors for the development of Plantar Fasciopathy, given that there are SO many, why are we so quick to blame one single factor?
That for many, may NOT be a problem!
Identified Risk Factors - Plantar Fasciopathy
↓
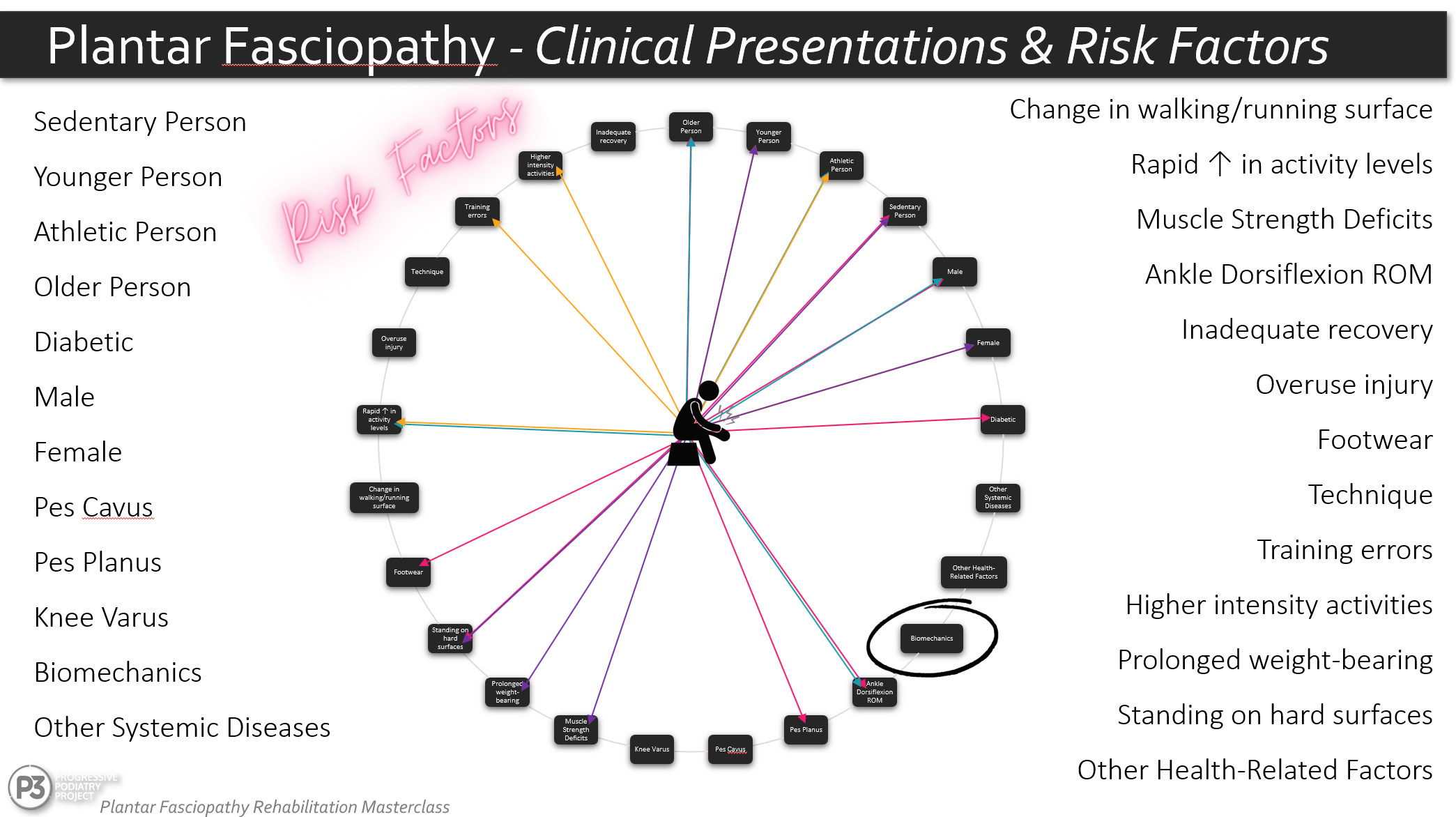
Note: There are 25 factors here (some aren't listed individually) - biomechanics = 1
We may have 4 different people with PF and 4 entirely different contributing factors.
Something to consider...
If you have a person presenting to your clinic with a chronic presentation (>3/12),
Could their gait be a result of the problem not the cause?
Yes, altering load orthomechanically may be something we need to address, regardless of cause or effect. BUT, if biomechanics aren't the 'root cause' or what we (may) need to address for more appropriate management, what do we do?
Don't jump into a gait &/or biomechanical assessment in the first 5 minutes
Instead...
Ask Better Questions → Get Better Results
By improving our clinical history taking and how we approach our initial consultations, there are two very positive things that can come out of it.
1) We are able to build an individual's clinical profile.
This means we are able to identify possible factors that are contributing to that individual's presentation and pathology. Which equates to implementing treatments/therapeutic interventions that are more likely to achieve a positive treatment outcome. Instead of throwing a handful of darts at a dartboard and hoping one sticks.
2) We are able to identify possible barriers to achieving our clinical outcomes.
Listening to not just WHAT they are saying, but HOW they are saying it, allows us to identify possible psychobehavioural barriers (ie: Yellow Flags) that may impact the formulation of our management strategy, as well as our clinical outcomes.
The first step is trying to figure out why something has developed in the first place, and is it something we can address?
The next step is trying to figure out if there are any factors that may impair our (and our client's) ability to address the problem/s? Whilst not all barriers are psychobehavioural, in chronic musculoskeletal pathologies it is always worth considering their potential presence.
A great place to start is with this paper by Matt Cotchett, Angus Lennecke & co, published in 2017
By sufficiently exploring a person's risk factors and the potential presence of psychobehavioural Yellow Flags, we are able to;
#1 Create more individualised management plans.
#2 Develop treatment narratives that will foster understanding, engagement & build positive therapeutic alliances.
#3 Not waste time, money and energy on assessments &/or therapeutic interventions that are not relevant &/or warranted in particular cases.
Remember...
The aetiology of Plantar Fasciopathy is a
multi-factorial interplay or mechanical load & individual risk factors.

Questions to Ask / Areas to Explore
To help you in building a more concise clinical profile...
#1 Activity History eg: sudden changes - sudden ↑ or ↓ in intensity/duration/frequency etc...
#2 Occupational History eg: activities at work, footwear at work, surfaces standing on etc...
#3 Social History eg: activities at home, footwear at home, stressors etc...
#4 Pain Pattern eg: location of pain, type of pain, alleviating &/or aggravating factors etc...
#5 Previous Treatments eg: what was done, what helped, what didn't help etc...
#6 Other Health Factors Hx eg: diabetes, systemic diseases, other injuries etc...
#7 Objective Tests eg: Windlass Tests, neural tests etc...
#8 Footwear eg: changes in footwear, work shoes, shoe rotation, sport shoes etc...
Final Thoughts
If we take the time initially to explore the background of a person & their pathology, we can avoid pigeonholing a them into what we assume is driving their pathology. This is arguably what can (& will create) more consistently positive outcomes and move us towards more person-centered care.
GO SLOW to GO FAST
That is, we don't need to go in guns blazing with a treatment intervention in the first 10 minutes of a consultation. By taking the time to explore the multitude of elements that make up a person's clinical presentation, we can actually fast-track recovery as we will be more targeted in our approach.
As always, I would love to hear your thoughts on this. Feel free to leave a comment or direct message me.
Also, if you are interested in learning more about this approach to Plantar Fasciopathy - P3's Plantar Fasciopathy Rehabilitation Masterclass will be launching soon. You can find out more here.
The aim of the course is to help clinicians build their knowledge, skills and confidence in creating individualsed management plans for their clients. We also work to build an understanding of when we may (or may not) need to prescribe exercises or implement load monitoring/modification strategies.
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
