
Do Reps Really Matter in Rehab?
Mar 29, 2022
Q: Do Repetitions Really Matter in Rehab?
A: Not always
When it comes to prescribing exercises and formulating rehabilitation programs, one of the biggest anxiety-inducing factors many clinicians face is the fear of getting it wrong.
This will often lead to one of three usual thought processes occurring.
- “I’ll just stick with 3 x 10, that seems to be a safe bet.”
- “Ummm… I literally have no idea, I’ll just refer on.”
- “I’m not really sure, but I know that *insert passive treatment modality* will usually make them feel better, so I’ll stick with that.”
Now there are instances where each of the above thought processes aren’t entirely wrong.
Yes, at times 3 x 10 is actually the dosage we should be prescribing.
BUT sometimes this can overdose a tissue, leading to an injury flare. OR it can underdose a tissue, leading to an increased susceptibility of re-injury occurring.
Yes, at times the best thing for the client is to refer them on to someone more suited to them or their pathology.
BUT sometimes you are the right person for them, you've just sold yourselves short.
Yes, at times passive treatment modalities can be beneficial in opening the treatment window.
BUT there should be a plan beyond the short-term symptom fix.
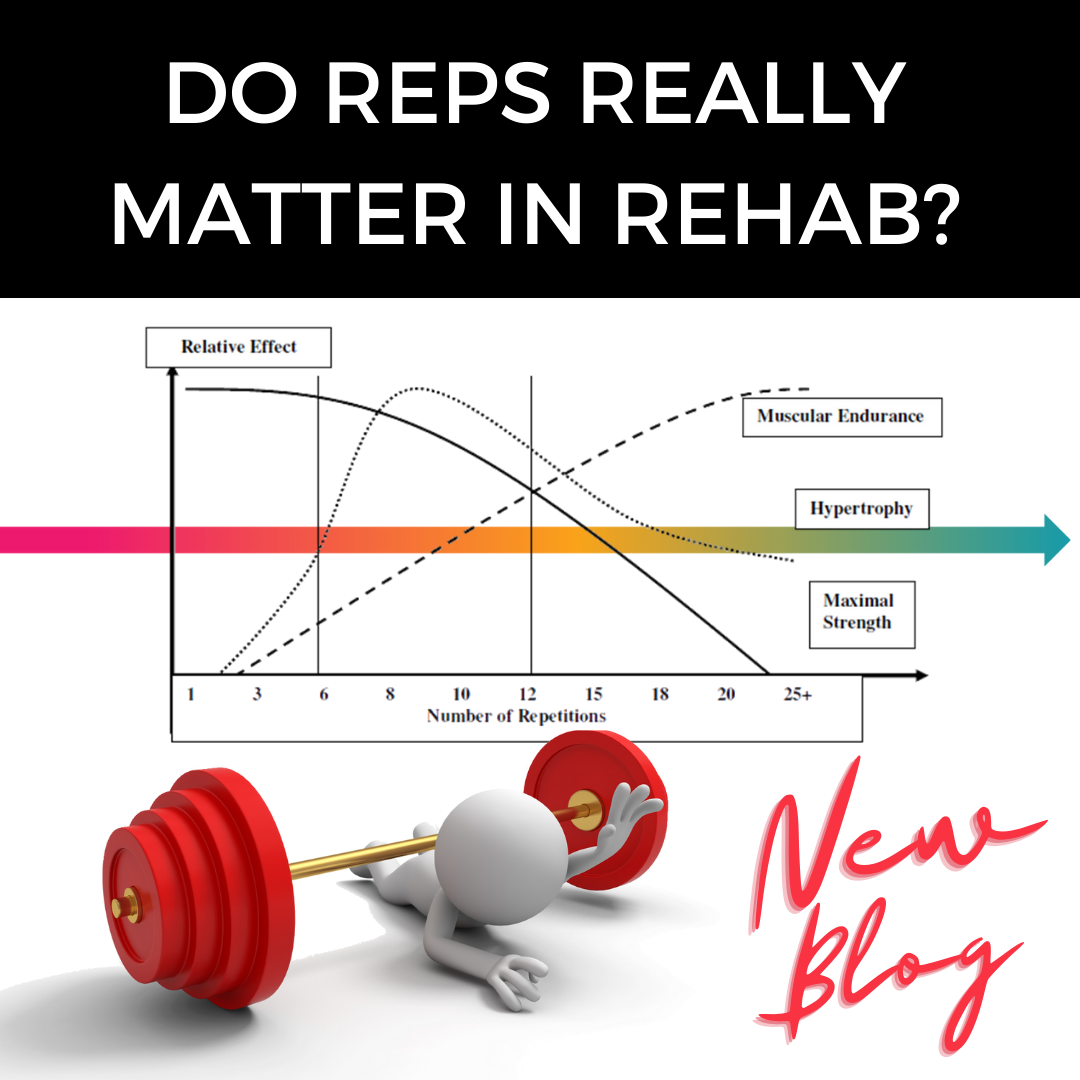
Now when it comes to repetitions in exercise, the number of repetitions performed tend to have differing effects on the body. This will impact how the body responds and adapts to the exercise immediately and in the roughly 72 hours after load exposure.
When we are progressing further through a rehabilitation program the dosage becomes, in my opinion, more important, all of which we will explore in future posts.
However during the early stages of rehabilitation I believe the magic number of repetitions for a rehabilitation exercise is…
The number of repetitions that can be done to achieve the therapeutic goal/s, without triggering a deleterious effect on the person &/or affected tissue.
Expanding upon this further is, the best exercise is the one that gets done.
Leaning on the literature a little to this point, we can look at the papers published by Michael Rathleff regarding High Load Strengthening for Plantar Fasciopathy.
Following-up from the initial paper, researchers reviewed the outcomes of self-determined vs self-dosed exercise, the results showed similar results at 12 weeks (references to articles below if you're interested).
When we consider the other elements of rehabilitation for a client, that being the psychobehavioural elements, the collaborative approach to exercise dosage is quite important.
Whilst some clients want to be told exactly what to do, others respond better to more of a framework and guidance.
When it comes to figuring out your approach to dosage for an individual, it can be tricky. However there are a few elements we can consider that may help guide us in this process.
What is their pathology &/or stage of tissue healing?
Always respect tissue healing time-frames!
What is the person’s movement literacy &/or history?
Have they had experience with exercise &/or rehabilitation before?
Are they someone who enjoys movement?
What is the person’s relationship to pain?
Is it healthy?
Do they have any maladaptive behaviours &/or beliefs around pain?
What are the overall goals of the treatment program?
Are we looking to return to activities of daily living or higher-intensity activities?
Whilst the above elements are by no means extensive, they are a good starting point to getting a feel of what your ‘dosage’ may look like.
The above factors can be very beneficial to us in the formative stages of our prescription writing. How do we then help our clients self-monitor and dose when they aren’t in the clinic with us?
I will often use the visual analog scale of pain (VAS-P).
During, after and the morning after a rehabilitation load exposure I educate my clients on following the numbers to determine their dosage.
0-3 good to go.
4-5 not great, but ok.
6-10 let's back it up.
Whilst the education I offer my clients is much more in-depth and tailored than the above, hopefully you get the idea.
Here's a snippet of the pain education flyer I use with my clients when helping them navigate their rehab in the presence of pain.
If you’d like to download my VAS-P education flyer to help with your client education & programming head to https://www.progressivepodiatryproject.com/pain to download your flyer today.
I hope this information has been helpful and I look forward to seeing you in the P3 Community.
References ↓
Rathleff MS, Mølgaard CM, Fredberg U, Kaalund S, Andersen KB, Jensen TT, Aaskov S, Olesen JL. High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up. Scand J Med Sci Sports. 2015 Jun;25(3):e292-300. doi: 10.1111/sms.12313. Epub 2014 Aug 21. PMID: 25145882.
Riel H, Jensen MB, Olesen JL, Vicenzino B, Rathleff MS. Self-dosed and pre-determined progressive heavy-slow resistance training have similar effects in people with plantar fasciopathy: a randomised trial. J Physiother. 2019 Jul;65(3):144-151. doi: 10.1016/j.jphys.2019.05.011. Epub 2019 Jun 13. PMID: 31204294.
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
