
When LESS is MORE in Rehab
Oct 20, 2022
When it comes to rehabilitating physical injuries, it can be very easy to fall into the trap of feeling like we have to DO something. Be it prescribing a range of rehabilitation exercises, to performing manual therapy or applying electrotherapies.
Whilst yes, at times any (or all) of those interventions may be warranted, what can be easy to forget is that for some clinical presentations less can really be more, if we are to achieve a positive treatment outcome.
Using the examples of plantar fasciopathy & Achilles tendinopathy, these are pathologies that often see structural changes & functional deficits occurring in the individual. However, it pays to remember there are a number of common subgroups of individuals who may develop these pathologies.

Abnormal exposure to mechanical loading will often result in structural changes to connective tissues, making them less load tolerant.
However, the tissue changes seen between these sub-groups that affect their load tolerance can vary, subsequently altering what we may need to advise/implement to assist in functional restoration.

In sedentary (+/- older &/or diabetic) individuals, the Achilles tendon and the plantar fascia may become stiffer, resulting in a tissue that can tolerate less strain &/or compressive loads before reaching a point of fiber stress and disruption. A number of processes are involved in the development of these stiffer connective tissues. For example, a theoretical process associated with these changes sees an increase in collagen cross-linking, developed as a result of increased advanced glycation end-products (AGEs) (Snedeker & Gautieri, 2014).
Whereas in active individuals with a presentation that may be more related to excessive loads being placed on a relatively healthy connective tissue structure, we may see increased proteoglycan content within the tissue. In a reactive phase of tendon pathology, the influx of proteoglycans is thought to increase the cross sectional area of the tendon, assisting in load distribution, among serving other functions related to remodeling - as proteoglycans play an important role in collagen fibrillogenesis.
Should high degrees of exposed load continue and sufficient time is not allowed for positive adaptation to occur, we may see a connective tissue structure with higher concentrations of substrates, enzymes &/or structural proteins resulting in the tissue being more compliant.
These differences in stiffness / compliance will impact the load exposures required to achieve the desired tissue adaptations for functional restoration to occur.
Both scenarios require time for adaptation to occur. However, what we do within that time is important and often varies.
How Does This Apply Clinically?
Load exposure (activities &/or exercises) and the subsequent dosage impact tissue adaptations that occur. Which means we firstly need to understand what is contributing to the individual's presentation, before we can implement a management plan.
Are they doing too much?
Are they not doing enough?
Are they too stiff?
Are they too compliant?
Secondly, we need to have an understanding of what the tissue needs to restore the ideal function for that individual.
The prescription & application load (ie: general movement, walking, running, stretching, isometrics, eccentrics &/or plyometrics) will all impact the resultant tissue stiffness / compliance adaptations of the exposed tissues.
To learn more about exercise prescription - click here
Q) How Can I Know When to Load or When to Remove Load?
A.i) Quite simply, your clinical history.
A.ii) Less simply, a client's clinical history + an understanding of the interplay of their individual risk factors in relation to the presenting pathology + the impact the pathology has on the function of the tissue.
Quite similar to the development of bone stress injuries, we may have a pathology that is fatigue/load related or insufficiency related (or potentially a combination of both).
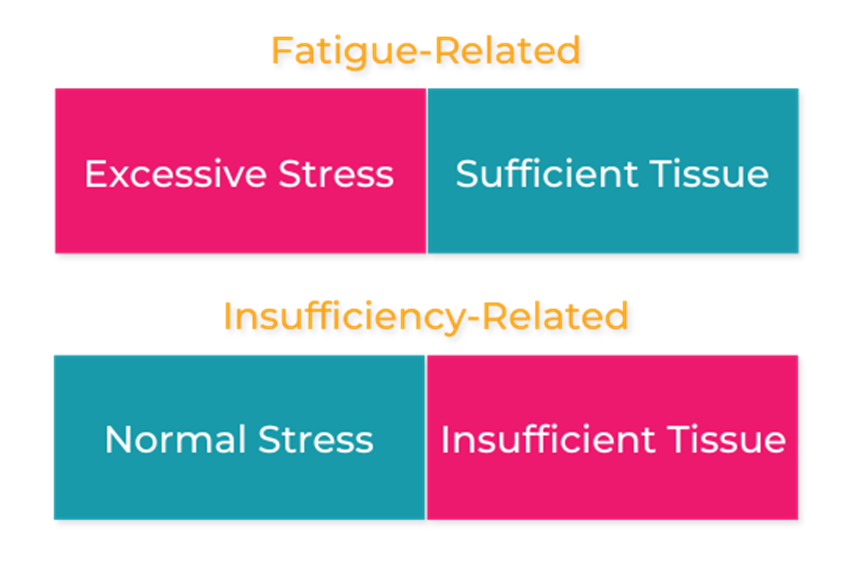
Fatigue/load related pathologies see relatively abnormal/excessive loads being applied to what would be considered 'normal'/healthy tissue, with sufficient load-tolerating capacity if excessive loads weren't present.
In contrast, insufficiency related injuries see relatively 'normal' loads being applied to tissues that do not have sufficient capacity to tolerate these loads, often resulting from inactivity &/or other health-related factors impairing the quality of the affected tissue/s. For example, reduced tissue integrity from ageing &/or diabetes. (we're not talking about BSIs here, we are talking tendinopathy &/or plantar fasciopathy)
If we are dealing with a fatigue-related pathology, simply reducing load and allowing sufficient time for adaptation to occur may be all that is required. If we are adding rehabilitation exercises into an already overloaded equation, we may simply exacerbate the problem.
However, if we are dealing with an insufficiency-related pathology, increasing load in a considered manner may be the optimal approach (+/- addressing modifiable factors contributing to their pathological presentation).
Side note: what may be required to 'calm things down' / manage symptoms / create an optimal environment for implementing load prior to 'building things up' in either scenario will vary between individuals, and we aren't exploring today.
Use the below table to visualise how the above examples re: application of load via rehabilitation exercises may further exacerbate a pathology ↓
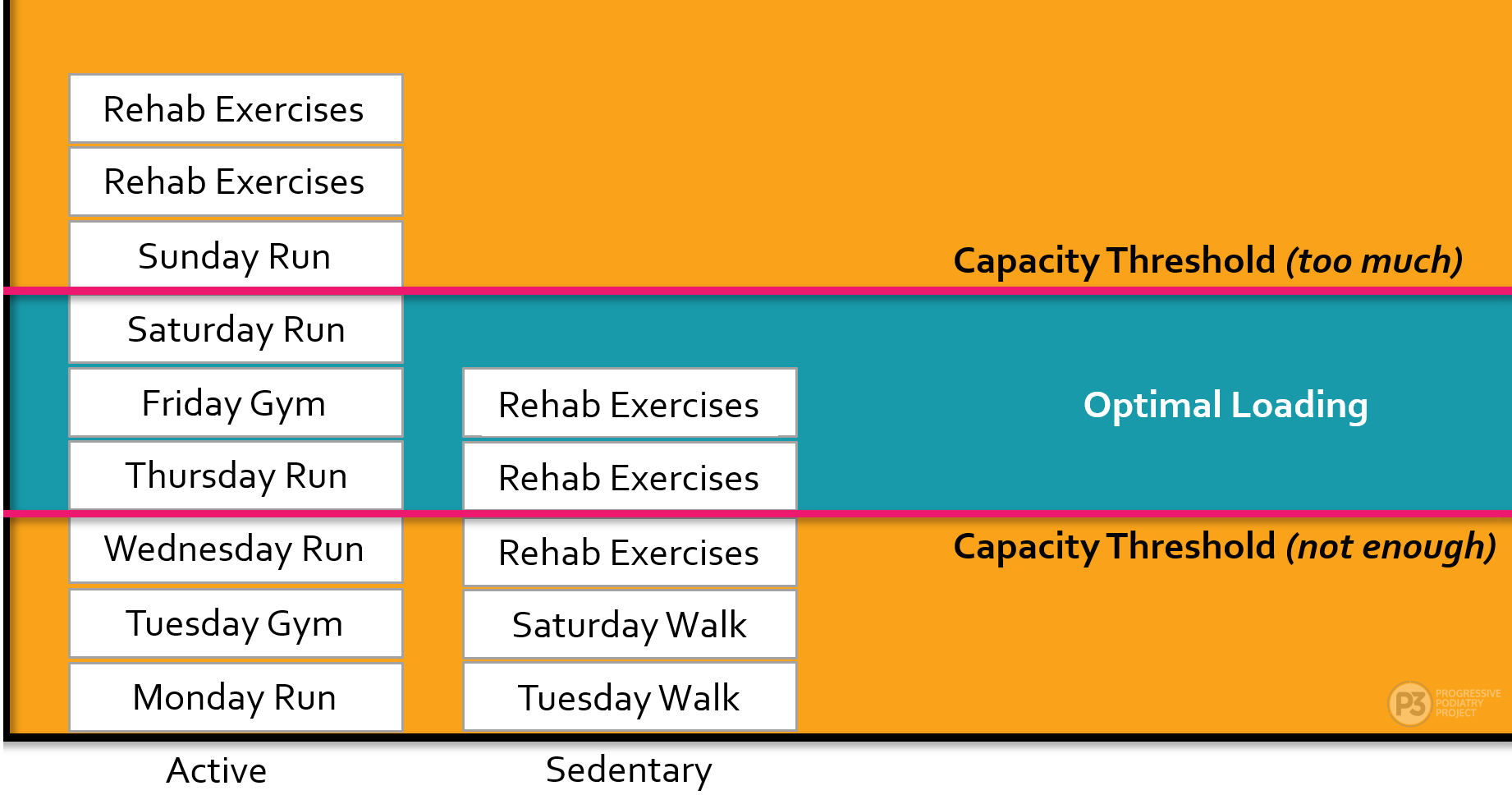
Whilst every client and their needs are different, the important take-home message here is that in order for our physical rehabilitation programs to be successful, we need to have an understanding of the load-capacity equation for that individual at that point in time.
Either way, we're wanting to achieve regular load exposure for sustainable, positive tissue adaptations. However, what's needed initially is where we find (and need) more nuance.
Removing load for a person who actually needs load to build their capacity can be detrimental to their outcomes.
In contrast, adding load to a person who actually needs to reduce load at that point in time to return to baseline, before we can look at strategies to build their sustainable capacity in the long-term can be equally detrimental.
My advice before you pull the trigger on an exercise prescription for Achilles tendinopathy or plantar fasciopathy presentation, is to ensure you've explored the person's clinical history enough to have an understanding of if you ADD load will it be adding to the problem?
As always, I'd love to hear your thoughts - comments or DMs are always welcome.
References
Juneja SC, Veillette C. Defects in tendon, ligament, and enthesis in response to genetic alterations in key proteoglycans and glycoproteins: a review. Arthritis. 2013;2013:154812. doi: 10.1155/2013/154812. Epub 2013 Nov 10. PMID: 24324885; PMCID: PMC3842050.
McMillan A, Landorf K, Gilheany M, Bird A, Morrow A, Menz H. Ultrasound guided corticosteroid injection for plantar fasciitis: a randomised controlled trial. J Foot Ankle Res. 2011 May 20;4(Suppl 1):O29. doi: 10.1186/1757-1146-4-S1-O29. PMCID: PMC3102950.
Parkinson J, Samiric T, Ilic MZ, Cook J, Handley CJ. Involvement of proteoglycans in tendinopathy. J Musculoskelet Neuronal Interact. 2011 Jun;11(2):86-93. PMID: 21625045.
Snedeker JG, Gautieri A. The role of collagen crosslinks in ageing and diabetes - the good, the bad, and the ugly. Muscles Ligaments Tendons J. 2014 Nov 17;4(3):303-8. PMID: 25489547; PMCID: PMC4241420.
Thorpe CT, Birch HL, Clegg PD, Screen HR. The role of the non-collagenous matrix in tendon function. Int J Exp Pathol. 2013 Aug;94(4):248-59. doi: 10.1111/iep.12027. Epub 2013 May 30. PMID: 23718692; PMCID: PMC3721456.
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
