
Utilising the Windlass Test to Guide Exercise Selection
Jun 12, 2023
How can we get more information, more individualisation & more consistent outcomes to our musculoskeletal management plans?
Read on...
In clinical practice there is often disconnect between various elements.
For example, diagnostic tests and exercise selection.
Many clinicians may utilise a test to identify what pathology they are dealing with, however, many stumble when it comes to figuring out the selection and timing of the therapeutic interventions that may be beneficial to aid their client's recovery.
This article hopes to guide you towards selecting more appropriate exercises for your clients with low load-tolerance suffering Plantar Fasciopathy.
How?
If we are prescribing exercises suited to the client's current load-tolerating capacity we can decrease the likelihood of over- or under-dosing our rehab (ie: prescribing exercises for PERSON with a pathology, as opposed to prescribing for a PATHOLOGY).
Yes, there will be plenty more articles on plenty more exercises - if you want to skip to knowing them all at once, check out the Plantar Fasciopathy Rehabilitation Masterclass here.
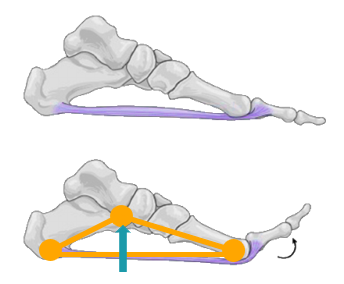
Firstly, what is the Windlass Test?
The Windlass Test was coined by Hicks in 1954.
In either a non-weight bearing or weight-bearing position a clinician will dorsiflex the hallux, with the hallux IPJ flexed - to take the FHL out of the equation, to engage the windlass.
This movement results in the plantar fascia winding around the metatarsal heals, subsequently shortening the distance between the heel and the forefoot, resulting in elevation of the medial longitudinal arch (Bolgla & Malone, 2004).
Clinical Utility
The Windlass Test is often used to aid in the diagnosis of Plantar Fasciopathy (or Plantar Fasciitis).
When pain is reproduced at the plantar medial calcaneal tubercle by performing the Windlass Test this is considered a positive test. This test is considered to have 100% specificity, but only 31.8% sensitivity (Bolgla & Malone, 2004).
Moving beyond utilising this test to tell us if a patient is experiencing Plantar Fasciopathy/Fasciitis, we can utilise this information to identify a potential starting point for physical rehabilitation (if it's required).
In 2015 Rathleff et al published a brilliant paper High-Load Strength Training Improves Outcome in Patients with Plantar Fasciitis (find it here).
As with many publications that take us a leap forward, a problem began where clinicians would begin prescribing almost all of their Plantar Fasciopathy patients the high-load strength training exercises.
The problem is that this exercise (like all exercises) can significantly overdose or underdose someone if we are not considering the client's current load-tolerating capacity.
This lead many clinicians that I have coached often asking themselves the question; "Does everyone need this exercises or does no one need it?" - the answer lies in the middle, some do, some don't.
If we are prescribing a HIGH-LOAD exercise to someone with LOW load-tolerating capacity, we're asking for a flare.
How can we improve our exercise prescriptions?
Focus on Function
Whenever we're prescribing an exercise we should have clear Therapeutic Goals in mind.
If we see someone with a presenting functional deficit, we should be aiming to restore their function (not just focus on pain!).
The first step is to understand the structure and function of the affected tissue.
Looking at the plantar fascia through the exercise prescription lens...
It is a tissue comprised primarily of Type I Collagen, that serves to absorb & release elastic strain energy to aid in propulsion during gait.
The underlying cause of plantar fasciopathy is thought to be similar to tendinopathy, with imaging & histopathological findings supporting this theory (Rajasekaran & Finnoff, 2015).
In the presence of Plantar Fasciopathy we often see a number of structural changes; angiofibroblastic hyperplasia - fibre disorientation, increases in myxoid ground substance, and an absence of inflammatory infiltrate to name a few (Reeve, 2022).
Given these changes often interfere with the tissue's ability to store & release mechanical energy, in addition to exhibiting a decrease in strain load tolerance, then it stands to reason that our therapeutic interventions should aim to address and improve these functional deficits.
How can we address this?
Exposure to mechanical loads that replicate the function of the tissue - in line with the current load-tolerating capacity.
ie: Strain loads and loads that require storage & release of mechanical energy.
A few questions we need to ask ourselves are;
- "What is my client's desired functional capacity?" (ask them about their goals).
- "What is their current functional capacity?" (gather subjective information & perform your clinical assessments).
- "How am I going to bridge the capacity gap?" (prescribe with purpose).
For some, exercise therapies won't be required. Load management, footwear, orthoses etc may be what comprises our management plan. For others, exercises can be highly beneficial in restoring function by triggering some of the positive tissue adaptations required to facilitate collagen remodelling.
If the Windlass Test yields a positive response, I would NOT begin with the High-Load Strengthening exercise, as this may overdose the loading of the tissue.
I would typically start with some low-load exercises, as a positive Windlass Test will demonstrate a low tolerance for strain loads.
- 1st MTPJ Stretching (left)
- 1st MTPJ Active ROM
- Seated Calf Raise (no-external resistance) aka Seated Active ROM. (middle)
- Heel Rocker (Weight Transition Focus) (right)

Eventually we may build up to the High-Load Strengthening, or we may simply program a gradual exposure to usual activities.
The main take-away here is that we;
a) Need to prescribe for the person (not just the pathology!).
b) Should be prescribing exercises that will address the functional deficits presenting.
c) Progress a client through exercises that replicate their goal function/activities.
d) Ensure that our exercises & dosages will apply sufficient stress to create positive adaptations in order for our client to tolerate the applied loads when we are returning them to their activities.
As always, I hope this has shared some insights into how we can utilise The Windlass Test beyond diagnostics.
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
