
Why Injuries Need Movement
May 23, 2022Is Your Decision to Immobilise Your Client's Injury Doing More Harm Than Good?
When it comes to managing musculoskeletal injuries, clinicians are often face a fear of causing further damage, or they are simply unsure how to navigate a client's rehab in the presence of pain.
This uncertainty can plague clinicians when managing both acute and chronic injuries, setting their clients up for frustration, poor treatment outcomes and possibly increasing the risk of re-injury.
Applying load to healing tissues can actually improve your rehabilitation outcomes. This may look like a faster return to work &/or sporting activities, not to mention a lower socioeconomic burden of the injury.
When we delay, avoid or under-dose loading an injury we can prolong the recovery process, in addition to impairing longer-term functional restoration. This applies to both acute & chronic injuries.
The consequence of delaying loading when managing an acute injury can result in longer recovery times and delayed return to sport/occupational activities.
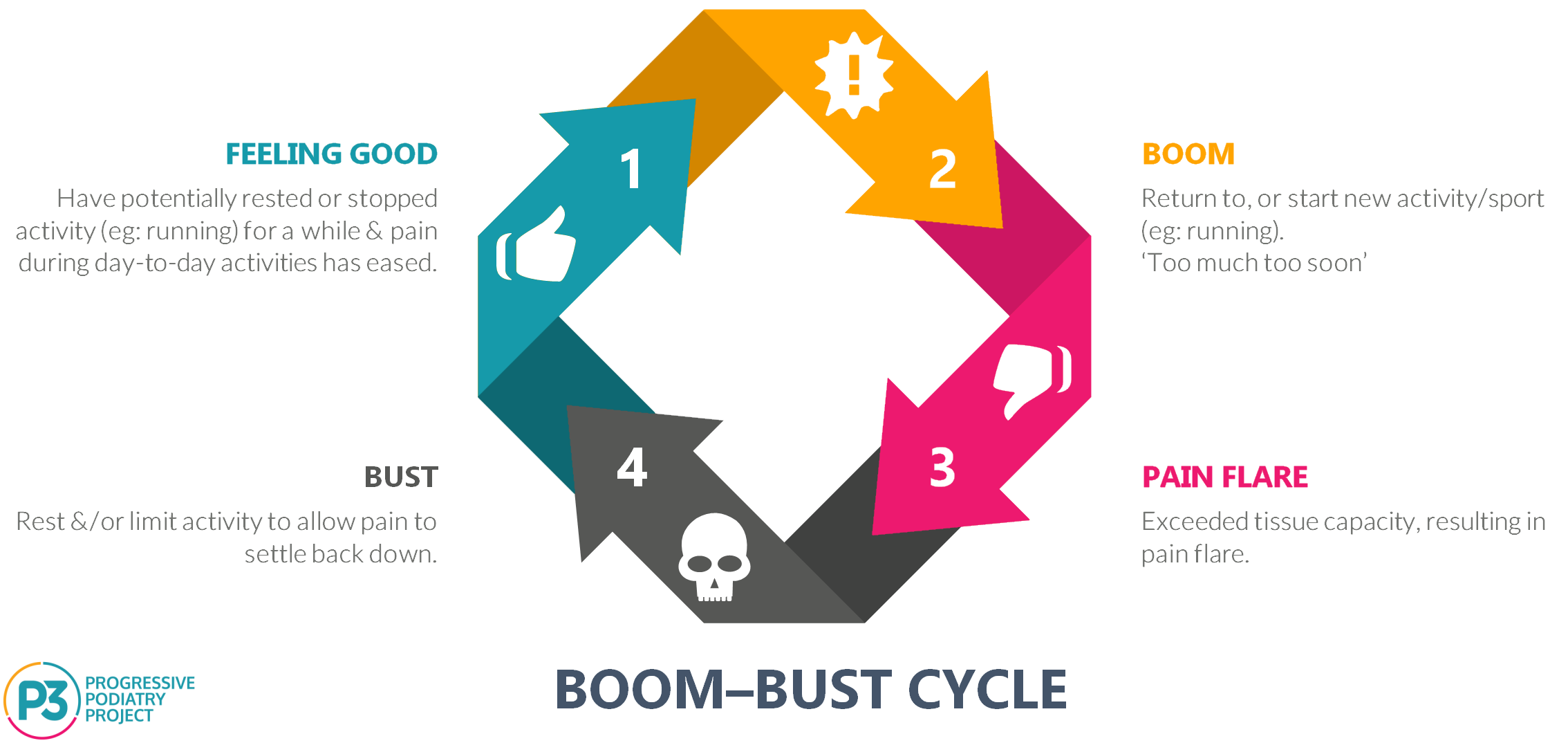
Similarly, when it comes to a fear of loading a chronic injury, for example Achilles tendinopathy &/or plantar fasciopathy, we can place a client at risk of falling victim of the boom-bust cycle.
Where clinicians often come undone, is that when it comes to chronic presentations of musculoskeletal injuries there is a failure to understand that;
Pain ≠ Tissue Damage
Advising rest or implementing a period of immobilisation may be a safe bet, because if you're not moving/loading you aren't going to engage in stimulus that can trigger pain.
However, whilst this is a safe bet, it is often short-changing your client's rehabilitation & functional restoration.
Yes, in some instance the amount of de-loading required can put a person in the immobilisation category. However, in the cases of chronic musculoskeletal presentations the number of people that actually need that level of de-loading is a lot less than we think.
De-loading to the minimum effective dose.
That is, we only need to reduce loading to a point where we open the window of opportunity for positive adaptation to begin.
Why Do Healing Tissues Need Load?
Mechanical Loading is a key determinant in maintaining connective tissue integrity.
This applies to ALL musculoskeletal tissues
BONES
TENDONS
MUSCLES
LIGAMENTS
Physiological loading triggers positive (or stable) tissue adaptation.
Overloading can induce progressive (or acute) microstructural damage & fatigue.
Absence of physiological stimulation leads to atrophy and degradation of tissue mechanical properties.

In the case of healing from an acute injury, loading is required to facilitate the organisation of newly forming connective tissues. This process commences as early as a few days after the initial injury event & is referred to as the proliferation phase.
The long-term benefits of early mobilisation after acute injuries & surgical repairs are well documented, for both tendon & ligament injuries.
For example;
"Joint immobilisation after mid-substance ligament rupture and during subsequent repair is known to produce healed ligament of smaller fibril diameter and poorer functional quality.
Thus, midsubstance tears are preferentially treated with partial immobilization casts and progressive remobilisation."
Doschak & Zernicke, 2005
In the case of remodelling a chronic injury, for example Achilles tendinopathy &/or plantar fasciopathy, our tissues are undergoing a constant state of turnover.
In many instances, tissue integrity can be restored with the introduction of physiological loading. The type of movement & the subsequent 'dosage' will vary between individuals. What we need to keep in mind is the above diagram regarding physiological loading. That is, we simply need to load enough to positively influence tissue adaptation.
In instances where tissue degeneration has evolved to a point physical restoration of the affected cells/structures may not be reversible (eg: tendon dysrepair), the remaining tissues can still positively adapt to load.
To review the the continuum model of tendon pathology head to ↓ https://bjsm.bmj.com/content/50/19/1187
Whilst damage to tissue structure may not be reversible in the cases of tendon dysrepair or some plantar fascia structural changes, functional restoration & improving load tolerating capacity still remain highly achievable therapeutic outcomes.
One of the most common barriers that presents to clinicians in these cases is as I mentioned, understanding how to navigate rehabilitation in the presence of pain. If you haven't checked it out yet, below is a link to a previous vlog where I explain how we can navigate our client's exercise rehabilitation in the presence of pain.
Video How to Navigate Rehab in The Presence of Pain (click image) ↓
Q: How Can We Improve Our Management?
A: Improve Our Knowledge.
I feel that in order for us to improve our injury management and make informed decisions regarding when to load & how much to load, there are a few knowledge gaps we need to fill.
- Improve our understanding of the phases of tissue healing.
- Improve our understanding of the mechanisms of pain generation.
- Understand how various musculoskeletal pathologies present (acute & chronic).
- Understand the tissue healing time-frames for various pathologies.
Regardless of the injury we are managing, there are a few golden rules we should follow.
The Golden Rules of Loading
Calm Sh*t Down, Build Sh*t Up
(Greg Lehman)
Load as much as you can,
as soon as you can.
Pain ≠ Tissue Damage in chronic injuries
I hope this article has given you some insight and guidance when it comes to approaching the management of musculoskeletal pathologies.
If you have found it helpful please share it with your network.
Are you a health practitioner who would like to improve your exercise prescription outcomes?
The Movement Prescription Blueprint is designed to help you do just that!
The MPB will help guide you through the exercise prescription process, allowing you to explore the 3 KEY elements of exercise prescription with your client, to help set you (and your clients) up for treatment success!
To download my FREE resource, The Movement Prescription Blueprint click HERE

If you want to improve your knowledge in regards to injury management & exercise prescription, our online course Exercise Therapies in Podiatric Practice will help you do just that!
Click below to take your exercise prescription to the next level!
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
