
Movement Alternatives to "Standard" Rehabilitation Exercises.
Jan 25, 2024
When we're in the initial stages of working with a client suffering a musculoskeletal injury, one of the hardest questions we can be faced with is;
"At this point in time does my client need to reduce or increase their load exposure?"
The reason this is such an important question to ask is that we know injuries need movement in order to facilitate the healing & functional restoration process, it's the timing and magnitude of load that we need to introduce that can often pose a problem.
When clients are self-managing their injury or a clinician lacks confidence in managing musculoskeletal pathologies, both can gravitate towards overdosing de-loading.
Moving beyond the question of adding or subtracting load, if we arrive at the decision to ADD load, the next question we must answer is;
"What loads do we need to apply and how can we go about this?"
Whilst some movements are considered "gold standard" in rehabilitation, for example, eccentrics for collagen remodelling &/or training dynamic range of movement.
There are a number of reasons in which a gold standard exercise may not be suitable, which leads to our last question that can often underpin how likely it is that a client will adhere to your prescribed program;
"Does my client require prescribed strengthening exercises or could they benefit from a dosed movement exposure?"
On the surface these may seem like they are the same thing, but how I want you to look at it is, differentiating from a scripted strengthening exercises (eg: a calf raise dosed at 4 sets of 10 reps) versus a dosed movement exposure (eg: walking 15 minutes 2 x per day or walking up & down 10 steps 3 x , twice per day).
There may be instances in which a dosed movement exposure may be more appropriate for our clients from an enjoyment, engagement & adherence perspective.
Whilst this approach isn't suited to every client, for many of our clients who require higher frequencies of low-dose movement, simply prescribing some dosed movement (+/- a considered footwear prescription) can be equally, if not more effective than a standard strength prescription.
What is Load in Rehabilitation?
In the context of rehabilitation, 'load' refers to the total amount of stress placed on the body. This includes not only physical load, but also factors like emotional stress and general lifestyle impacts.
Loads can be mechanical, physiological and psychological.
Mechanical Load
Mechanical load refers to the physical forces exerted on the body during activities.
This includes forces acting on muscles, bones, tendons, ligaments and joints resulting from movement and gravity.
Key Characteristics
Types of Forces/Loads: Compressive, tensile, and shear forces.
Impact on Tissues: Mechanical load triggers cell signalling and cellular responses via mechanotransduction. These responses can result in either positive or negative adaptations of our connective tissues.
Positive adaptation = building capacity.
Negative adaptation = injury &/or losing capacity.
Relevance in Rehab: Understanding mechanical loads is vital for rehabilitation programming. This allows us to match movement prescriptions to current capacity, as well as developing a roadmap for returning our injured clients to their desired activities.
Underloading (then loading) & overloading (&/or under-recovery) can lead to the development of musculoskeletal injuries.

Whereas appropriate loading is necessary for facilitating recovery, improving strength/motor control/endurance/power and reducing the risk of future injuries.

Physiological Load
Physiological load encompasses the internal bodily responses to physical activity and mechanical loads.
This includes cardiovascular, respiratory, metabolic, and hormonal responses.
Key Characteristics
Systemic Response: In response to physical activity and mechanical loads, we may observe changes in heart rate, blood pressure, oxygen consumption, and energy expenditure.
Adaptation Over Time: With regular exercise and sufficient time to recover, the body adapts, leading to improved endurance, efficiency, and recovery.
Relevance in Rehab: Monitoring physiological responses to activity and mechanical load can give an indication of an individual's training load. Understanding these responses can be an important element for injury risk reduction and performance programming.

Psychological Load
Psychological load refers to the mental and emotional aspects of physical activity and/or responses to injury.
Elements that comprise psychological load includes motivation, stress, mental fatigue, and the overall psychological impact of injury and rehabilitation.
Key Characteristics
Cognitive and Emotional Factors: Stress levels, anxiety, motivation, and enjoyment.
Impact on Performance and Recovery: Psychological state can influence pain perception, adherence to rehab, and overall well-being.
Relevance in Rehab: Recognising the psychological load is crucial for a holistic approach to rehabilitation. Addressing psychological barriers can improve adherence to rehab programs and overall recovery outcomes.

Diving deeper into the aforementioned elements, yellow flags (ie: psychobehavioural factors) can significantly impact a client's recovery from a musculoskeletal injury.
From Exercise Therapies in Podiatric Practice (2022)
For the purpose of our exploration of today's question "Does my client require prescribed strengthening exercises or a dosed movement exposure?", we will be focusing on mechanical and psychological elements that may help...
Closing the Capacity Gap
Rehabilitating musculoskeletal pathologies essentially boils down to closing the capacity gap.
![]()
A capacity gap exists where the loaded tissues simply don't have the ability to tolerate the applied loads and/or an individual has psychological elements/barriers to movement that may predispose or result from injury.
Psychobehavioural barriers (aka Yellow Flags) can present concurrently with a mechanical tolerance deficit, develop as a result of a mechanical tolerance deficit (acute or chronic injury), or present independently.
Some of the most common yellow flags that may present are pain catastrophising, kinesiophobia and fear-avoidance behaviours, all of which can signifiantly impact rehabilitation outcomes.

"Catastrophising is associated with reduced likelihood for exercise and implementing positive behaviour patterns." Cotchett et al (2017)
How & Why Can We Use 'Dosed Movement' in lieu of Prescribed Strengthening in Rehab?
Whilst there are a number of "gold standard" exercises for various musculoskeletal pathologies, for example; eccentric calf raises for Achilles tendinopathy (more on current concepts for Achilles tendinopathy rehab here).
There may be instances in which many gold standard exercises may overdose a client's rehabilitation, as well as instances in which a client simply won't do your prescribed exercises due to any number of reasons.
These reasons can be (but not limited to);
-
Low motivation.
-
Negative previous experiences.
-
Client preferences.
-
Low movement literacy.
-
Low levels of self-efficacy.
-
Access to equipment.
-
Belief the exercises may cause more harm or not provide benefit.
As much as it may be frustrating when a client won't adhere to a prescribed exercise plan, there are a number of ways in which we can introduce therapeutic movement and facilitate functional restoration and close the capacity gap.
The good news is that all types of movement will stimulate cellular changes that can be beneficial for tissue remodelling, it just depends on the individual & the level of tolerance of the tissue/s.
The therapeutic effect comes when the exercise or movement is within the tissue's window of tolerance, applies sufficient stress to stimulate a positive response (without overdosing), and the tissue is allowed sufficient time to adapt to the applied load.
For some, low-grade stretching may apply enough load to stimulate positive tissue adaptations, for others, plyometrics or heavy-slow resistance may be required to achieve the desired tissue response.
Poblems arise when a prescribed exercise does not align with a client's current capacity and/or does not align with guiding them towards their desired capacity.
Instead of asking "What's the best exercise for ____________ pathology?"
Possibly a better way of thinking is asking "What loads do the tissues need to be exposed to that will trigger the required adaptations to close my client's capacity gap?"
Now, if we have someone who is wanting to return to high-load activities, we may need to prescribe specific dosed exercises to restore their functional capacity.
However, if we have a client who is simply wanting to return to their activities of daily living (ADLs) and/or low-load activities such as walking, we may be able to prescribe dosed movement/activity exposure to build the tolerance.
Again, it will depend on how large the capacity gap is, your clinical reasoning and the client you are working with.
Below is an adaptation from the Baxter paper (2021), where the authors provided a concise overview of exercises that progressively load the Achilles tendon.
It is one of the easiest ways in which we can illistrate how & why many rehabilitation programs can fail to build sufficient capacity to return a client safely to their desired activity. It also illistrates how selecting exercises based on pathology irrespective of considering individual capacity can overdose a prescribed exercise.
The selection of an exercise coupled with its subsequent "dosage" and prescribed in consideration to the current load-tolerance is the required approach for many musculoskeletal rehabilitation programs.
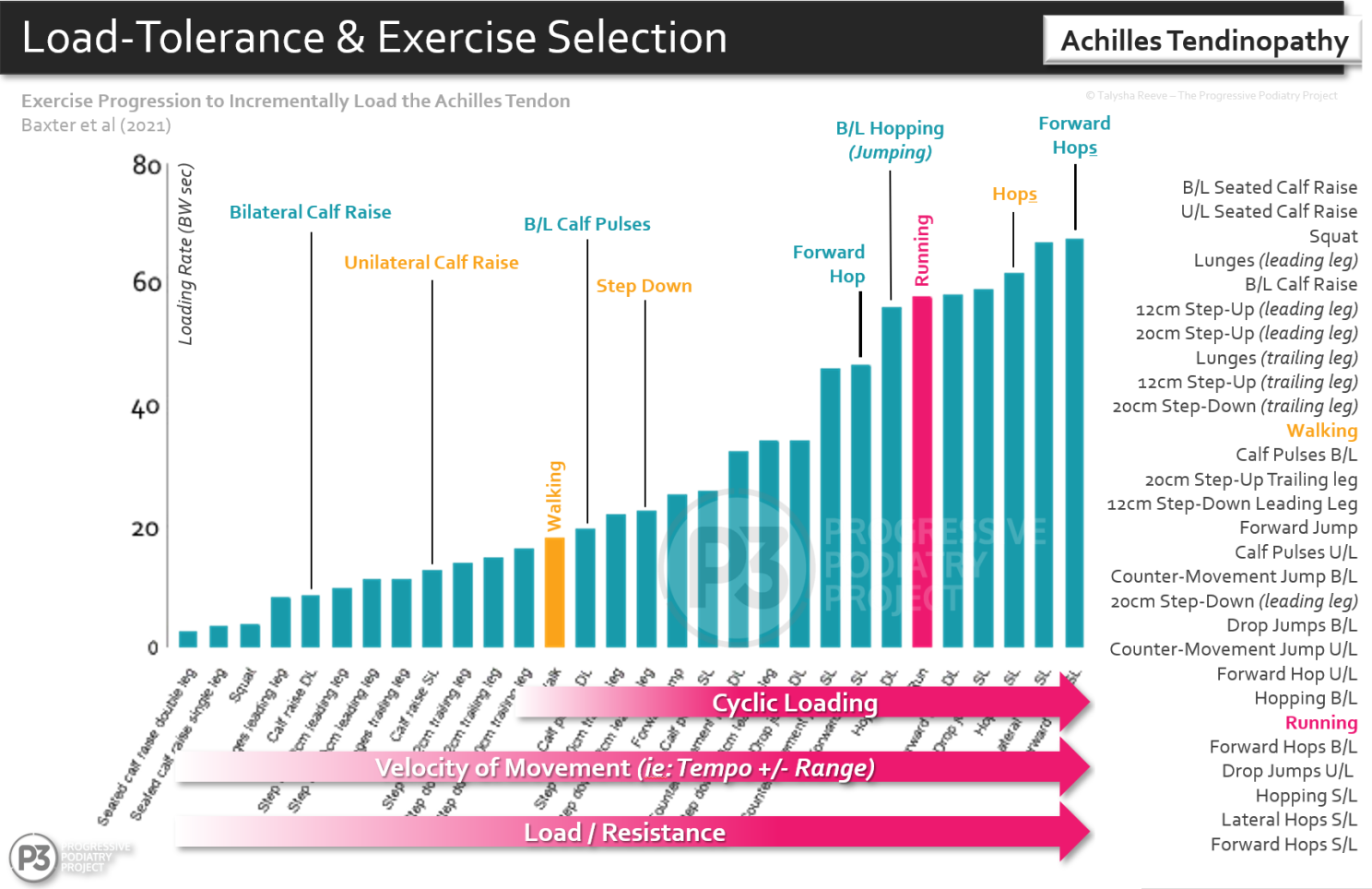
Exercise Therapies in Podiatric Practice Lecture Slide - Adapted from Baxter et al (2021)
When we are dealing with clients wanting to return to high-load activities or sports, such as distance running, AFL etc, it often isn't these clients that we experience the most difficulties with when it comes to engaging in and adhering to prescribed "typical" strength exercises for their rehabilitation.
Remembering that both active and sedendary invidivuals can develop musculoskeletal pathologies, including Achilles tendinopathy and plantar fasciopathy, it can be clients at the other end of the spectrum that clinicians experience difficulty achieving "buy-in" to their rehabilitation programs.
If we have a client with a relatively sedentary lifestyle, limited exposure to physical activity, limited movement literacy, and/or low motivation to engage in physical activity, prescribed strengthening exercises may be difficult to foster engagement in - even for clinicians experienced in exercise prescription and managing musculoskeletal pathologies across diverse client groups.
The best exercise? The one that gets done!
In order for us to be able to prescribe a movement exposure program we need to ask ourselves a number of questions.
-
What is the current load tolerating capacity of the tissue?You may gather this information from a combination of clinical history taking and your clinical assessment.For example; gathering information about what movements/activities aggravate and/or alleviate.
-
What movements can the client do that fit within their preference, daily schedule and their load tolerating capacity?Are they able to engage in some walking before symptoms flare? (eg: can walk 20 minutes daily with no problem, yet 30 minutes may be too much).
-
Are there any elements of the movement exposure that we may need to/be able to modify via other means to widen the therapeutic window to facilitate engaging in movement?This may be the utilisation of footwear and/or orthoses to modify mechanical loads. For example; a client with posterior tibial tendon dysfunction (PTTD) stage I or II, may benefit from footwear with a higher heel pitch, medial support, a higher degree of midsole bending stiffness +/- an orthotic device.
-
Am I able to explain the parameters for overdosing & underdosing this movement exposure to my client and they understand it?This will often involve conveying the importance of movement as part of their rehabilitation and also ensuring the client understands their dosage parameters. The Traffic Light System is an easy-to-understand method for educating clients to try and keep consistent movement exposure within their window of tolerance.
-
Will this movement exposure build sufficient capacity for their desired movement/functional goals?If you are prescribing walking +/- footwear for someone looking to return to AFL football, then likely not. However, if you are prescribing walking +/- footwear for someone who will only be returning to walking & activities of daily living (ADLs), then the answer is possibly yes.
The next step to understanding how this approach can work is gaining an understanding of the "dosage" parameters of walking/running (or other movement exposures that you are considering).
When it comes to strength training we have our dosage parameters (more on this here), yet many clinicians can struggle with understanding walking/running "dosage" (AFHP's Running Rehab - Understanding "Dose" explores this in-depth).
To get started, things you will want to consider relating to walking or running "dosage" are; time, distance, pace & elevation.
There are other elements that comprise running dose, but for the purpose of this article we'll focus on these 4.
Then you may need to consider footwear construction elements that may influence the fit, feel & function of a shoe (more on this here).
What Can a Movement Exposure "Dosage" Look Like?
Example 1: An older, relatively sedentary client with mid-portion Achilles tendinopathy requires Achilles loading for tendon remodelling & building capacity. As well as exercises to improve plantar flexion strength & increase ankle dorsiflexion ROM, yet keeps forgetting to do their rehab &/or doesn't want to.
You may have ascertained a movement tolerance of 6 unilateral calf raises before pain increases to 4-6/10 (VAS-P) via your clinical assessment.
You may ask them if they have any stairs at home or nearby or a sloped surface (eg: driveway), if they do you may prescribe some trips up and down the stairs/driveway in lieu of calf raises.
Let's say they have a set of 4 steps at home or a 15m sloped driveway on a roughly 10 degree pitch.
Utilising the Traffic Light System you may prescribe 5 "sets" of walking up & down their stairs (up & down 5 times in a row) twice per day.
You could also prescribe walking up & down the driveway 3-4 x twice per day.
You may consider the footwear they are performing these activities in (heel pitch, forefoot rocker, midsole bending stiffness etc).
As a progression, the number of repetitions (laps) and/or walking speed may be increased.
Example 2: A client with plantar fasciopathy, wanting to return to ADLs & who would benefit from tensile load exposure as they engage in infrequent loading, thus requires introduction of long-term, low-dose, high-frequency movement exposure.
You may have ascertained a movement tolerance of 8 bilateral high-load plantar fascia calf raises before pain increases to 4-6/10 (VAS-P) via your clinical assessment.
You may have gathered from their clinical history that they do very little day-to-day walking activities and once per week go shopping or for a long walk, resulting in a pain flare.
In lieu of high load plantar fascia strengthning you may prescribe 5-10 minutes of daily, continuous walking in a minimal style shoe to introduce regular load exposure.
You may utilise the Traffic Light System to monitor time exposure, in order to progress or regress the daily walking time.
The minimal style of shoe will have a low heel pitch and low degree of midsole bending stiffness allowing tensile loading of the plantar fascia (one study investigated minimal footwear & pain reductions in plantar fasciopathy here).
Initially, you may recommend walking on flat surfaces for 5-10 minutes once per day in the desired shoes.
As a progression, the duration of walking (minutes), the frequency of walking (daily, multiple times per day etc), and/or elevation (hills) may be increased. As well as increasing time in the shoes with minimalist characteristics.
Bear in mind these approaches aren't for everyone, though it can be a perfect approach for some.
Please ensure you conduct a thorough assessment, apply clinical reasoning, and ensure you and your client are on the same page when it comes to understanding the role of the therapeutic interventions & "dosages".
One of our recent webinars as part of Athletic Footwear for Health Professionals explores this entire concept in-depth, in the webinar Footwear Prescription for Plantar Fasciopathy - Prescribing with Purpose.
If we have a thorough understanding of footwear construction elements that may influence the fit, feel & function of a shoe, we can utilise footwear as an effective treatment tool when combined with a load exposure program.
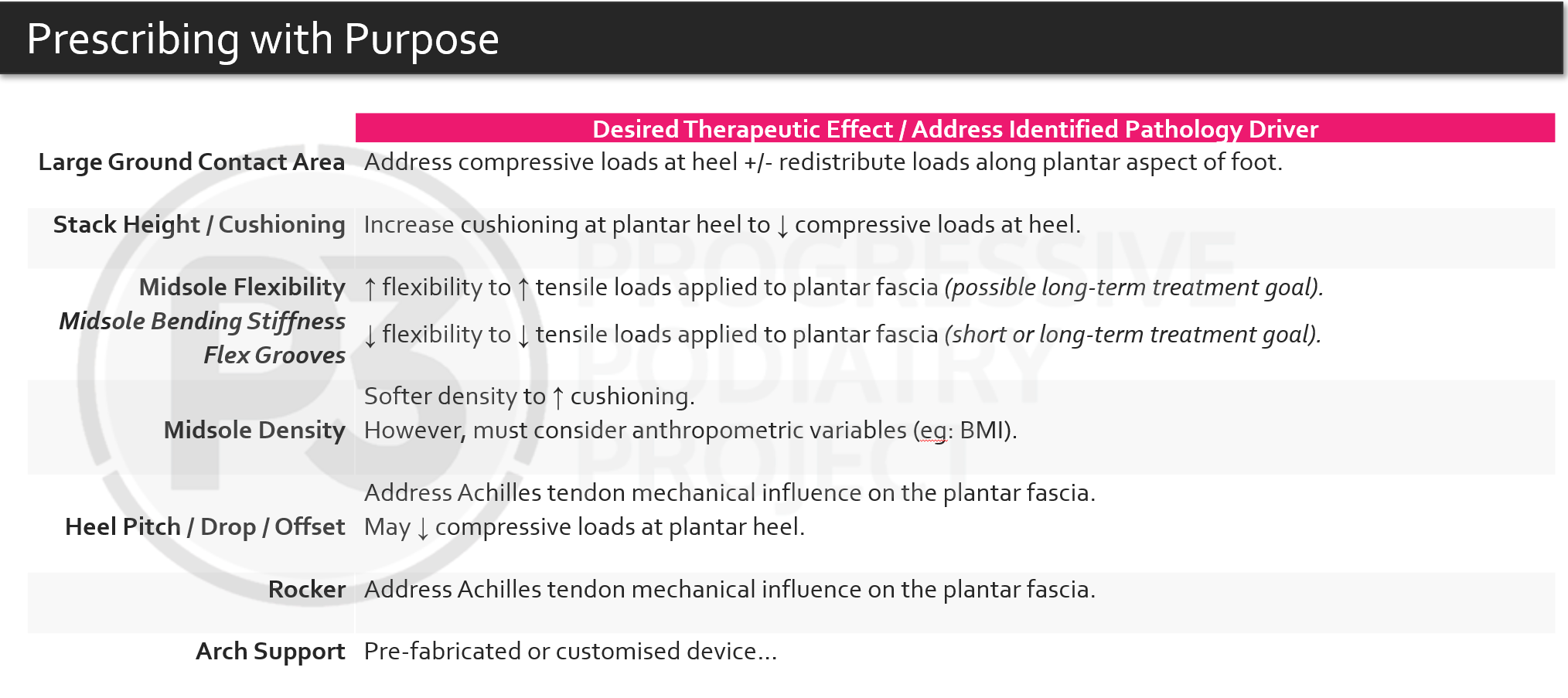
Footwear construction elements that may assist managing Plantar Fasciopathy (P3 - 2023)
As I mentioned, these approaches certainly aren't for everyone, though they can be highly beneficial to those clients who are resistant (for whatever reason) to "typical" rehab, whose capacity (current & desired) aligns with this approach and whose long-term management of the condition somewhat boils down to needing higher frequencies of lower-dose movement.
If you'd like to learn more I encourage you to check out our online education courses or live events that we will be running in 2024 - info here.
As always, I'd love your thoughts on this article.
Do you feel this information will help you in your clinical practice?
Join the Research Round-Up
Free monthly newsletter, delivering the latest research straight to your inbox
Research Round-Up delivered at the end of each month
